
Relationship between NLR, CA19-9/GGT ratio and preoperative microvascular invasion in hepatocellular carcinoma
-
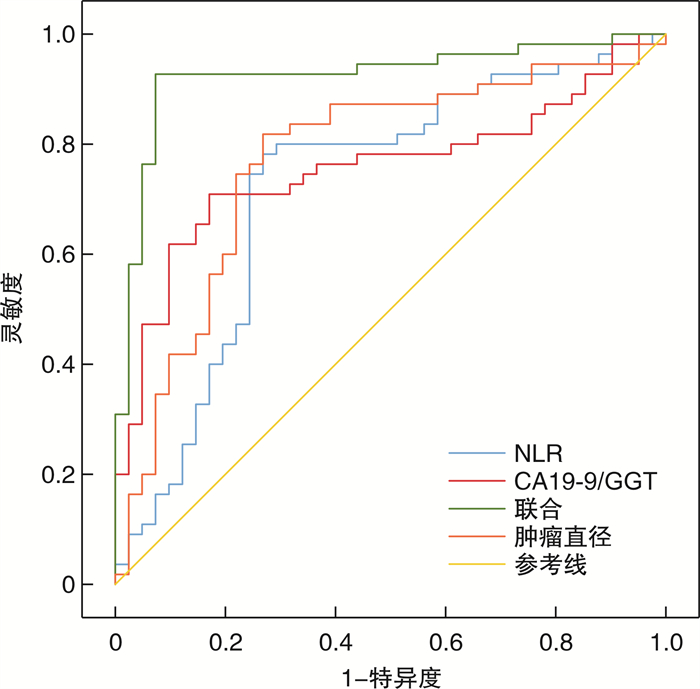
摘要: 目的 探讨中性粒细胞和淋巴细胞比值(NLR)、癌胚抗原19-9(CA19-9)/γ-谷氨酰转肽酶(GGT)比值与肝细胞癌(HCC)术前微血管侵犯(MVI)的关系。方法 回顾性选择2016年1月—2022年1月南京医科大学附属淮安第一医院收治的96例HCC患者,根据术后病理提示是否发生MVI将患者分为MVI组(55例)和非MVI组(41例)。收集患者人口学资料、术前超声影像学资料和实验室数据,术后病理资料,计算术前NLR以及CA19-9/GGT比值。多因素logistic回归分析NLR、CA19-9/GGT比值与HCC术前MVI的关系。绘制受试者工作特征曲线(ROC),分析NLR、CA19-9/GGT比值预测HCC患者术前发生MVI的价值。结果 MVI组肿瘤直径、NLR、CA19-9/GGT比值大于非MVI组(P< 0.05),血流信号Ⅱ~Ⅲ级比例、Edmondson-Steiner分级Ⅲ~Ⅳ级比例,TNM分期Ⅲ~Ⅳ期比例,血管侵犯比例高于非MVI组(P< 0.05),肿瘤数目多于非MVI组(P< 0.05)。肿瘤直径、NLR、CA19-9/GGT是HCC患者术前发生MVI的危险因素(P< 0.05)。联合NLR、CA19-9/GGT比值、肿瘤直径预测HCC患者术前发生MVI的曲线下面积为0.924,高于单独NLR、CA19-9/GGT比值、肿瘤直径的0.756、0.723、0.772(z=3.911、3.470、3.182,P< 0.05)。结论 高NLR、CA19-9/GGT比值与HCC术前发生MVI有关,在HCC术前MVI预测中具有较高的价值。Abstract: Objective To investigate the relationship between neutrophil/lymphocyte ratio(NLR), carcinoembryonic antigen 19-9(CA19-9)/gamma-glutamyl transpeptidase(GGT) ratio and microvascular invasion(MVI) before hepatocellular carcinoma(HCC).Methods Clinical data of 96 HCC patients admitted to our hospital from January 2016 to January 2022 were retrospectively selected, and the patients were divided into MVI group(55 cases) and non-MVI group(41 cases) according to postoperative pathological findings. Demographic data, preoperative ultrasound imaging data, laboratory data, and postoperative pathological data were collected, and preoperative NLR and CA19-9/GGT ratio were calculated. The relationship between NLR, CA19-9/GGT ratio and MVI before HCC was analyzed by multivariate logistic regression analysis. Receiver operating characteristic curve(ROC) was drawn to analyze the value of NLR and CA19-9/GGT ratio in predicting the occurrence of preoperative MVI in HCC patients.Results Tumor diameter, NLR and CA19-9/GGT ratio in MVI group were higher than those in non-MVI group(P< 0.05), the proportion of blood flow signal gradeⅡ to Ⅲ, Edmondson-Steiner grade Ⅲ to Ⅳ, TNM stage Ⅲ to Ⅳ, and the proportion of vascular invasion were higher than those in non-MVI group(P< 0.05). The number of tumor was higher than that of non-MVI group(P< 0.05). Tumor diameter, NLR and CA19-9/GGT were risk factors for preoperative MVI in HCC patients(P< 0.05). The area under the curve for predicting preoperative MVI in HCC patients by combining NLR and CA19-9/GGT ratio was 0.924, which was higher than 0.756, 0.723 and 0.772 of NLR, CA19-9/GGT ratio and tumor diameter alone (z=3.911, 3.470, 3.182;P< 0.05).Conclusion High NLR and CA19-9/GGT ratio are associated with the occurrence of MVI before HCC, and have high value in the prediction of MVI before HCC.
-

-
表 1 两组患者基线资料比较
例(%) 组别 MVI组(n=55) 非MVI组(n=41) t/z/χ2 P 年龄/岁 55.12±17.03 56.02±17.28 0.255 0.800 性别 0.206 0.650 男 31(56.36) 23(56.10) 女 24(43.64) 18(43.90) HCC病因 0.442 0.979 肝硬化 19(34.55) 16(39.02) 乙型肝炎 14(25.45) 11(26.83) 酒精性肝病 13(23.64) 8(19.51) 非酒精肝病 7(12.73) 5(12.20) 其他 2(3.63) 1(2.44) 肿瘤直径/cm 6.02(4,8) 4.08(2,6) 7.704 < 0.001 肿瘤数目/个 3.67(1,5) 2.91(1,4) 3.998 < 0.001 内部回声 0.456 0.796 高回声 21(38.18) 18(43.90) 低回声 19(34.55) 14(34.15) 等回声 15(27.27) 9(21.95) 血流丰富程度分级 4.856 0.028 0~Ⅰ级 16(29.09) 21(51.22) Ⅱ~Ⅲ级 39(70.91) 20(48.78) Edmondson-Steiner分级 5.151 0.023 Ⅰ~Ⅱ级 22(40.00) 26(63.41) Ⅲ~Ⅳ级 33(60.00) 15(36.59) TNM分期 4.954 0.026 Ⅰ~Ⅱ期 25(45.45) 28(68.29) Ⅲ~Ⅳ期 30(54.55) 13(31.71) 血管距离肿块最近距离 4.526 0.033 ≥1 cm 28(50.91) 12(29.27) < 1 cm 27(49.09) 29(70.73) Child-Pugh分级 1.043 0.307 A级 39(70.91) 25(60.98) B级 16(29.09) 16(39.02) 肝炎分级 0.398 0.819 G0~1 14(25.45) 9(21.95) G2 22(40.00) 19(46.34) G3~4 19(34.55) 13(31.71) 纤维化分期 0.135 0.935 S0~1 12(21.82) 9(21.95) S2 21(38.18) 17(41.46) S3~4 22(40.00) 15(36.59) ALT/(U·L-1) 79.26±12.35 78.65±13.26 0.232 0.817 AST/(U·L-1) 69.82±10.47 68.09±12.37 0.741 0.461 AFP 16.356 < 0.001 ≥200 μg/L 39(70.91) 12(29.27) < 200 μg/L 16(29.09) 29(70.73)  下载: 导出CSV
下载: 导出CSV
表 2 MVI组和非MVI组NLR、CA19-9/GGT比值差异
X±S 组别 例数 NLR CA19-9/GGT MVI组 55 3.02±0.74 2.75±0.61 非MVI组 41 2.16±0.43 1.81±0.42 t 6.647 8.477 P < 0.001 < 0.001
下载: 导出CSV
表 3 HCC患者术前发生MVI的logistic回归方程
因素 β SE Wald χ2 OR(95%CI) P 常数项 7.152 1.956 13.370 - < 0.001 肿瘤数目 0.206 0.191 1.163 1.229(0.845~1.787) 0.331 血流丰富程度分级 0.053 0.041 1.671 1.054(0.973~1.143) 0.531 Edmondson-Steiner分级 0.105 0.096 1.196 1.111(0.920~1.341) 0.462 TNM分期 0.043 0.039 1.216 1.044(0.967~1.127) 0.479 血管距离肿块最近距离 0.211 0.203 1.080 1.235(0.830~1.838) 0.326 AFP 0.175 0.163 1.153 1.191(0.865~1.640) 0.405 肿瘤直径 0.853 0.251 11.549 2.347(1.435~3.838) < 0.001 NLR 0.603 0.179 11.348 1.828(1.287~2.596) < 0.001 CA19-9/GGT 0.511 0.163 9.828 1.667(1.211~2.294) 0.003
下载: 导出CSV
表 4 NLR、CA19-9/GGT比值、肿瘤直径预测HCC患者术前发生MVI的效能
因素 曲线下面积(95%CI) P 灵敏度/% 特异度/% 约登指数 肿瘤直径 0.772(0.675~0.851) <0.001 81.82 73.17 0.5499 NLR 0.756(0.658~0.838) <0.001 74.55 73.17 0.4772 CA19-9/GGT 0.723(0.622~0.809) <0.001 70.91 80.49 0.5140 联合 0.924(0.852~0.968) <0.001 92.73 92.68 0.8541
下载: 导出CSV
-
[1] 张为, 范恒亮, 李榕华. 经肝动脉化疗栓塞治疗小于5 cm单发肝细胞癌的临床效果及其影响因素分析[J]. 现代消化及介入诊疗, 2020, 25(5): 662-665. doi: 10.3969/j.issn.1672-2159.2020.05.026
[2] Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6): 394-424. doi: 10.3322/caac.21492
[3] Yang L, Gu D, Wei J, et al. A Radiomics Nomogram for Preoperative Prediction of Microvascular Invasion in Hepatocellular Carcinoma[J]. Liver Cancer, 2019, 8(5): 373-386. doi: 10.1159/000494099
[4] Jiang YQ, Cao SE, Cao S, et al. Preoperative identification of microvascular invasion in hepatocellular carcinoma by XGBoost and deep learning[J]. J Cancer Res Clin Oncol, 2021, 147(3): 821-833. doi: 10.1007/s00432-020-03366-9
[5] 吴晓龙, 毕新宇, 李智宇, 等. 术后中性粒细胞和淋巴细胞比值与肝细胞癌切除术后复发及患者生存的关系[J]. 中华肿瘤杂志, 2018, 40(5): 365-371. doi: 10.3760/cma.j.issn.0253-3766.2018.05.009
[6] Lyu SC, Wang J, Huang M, et al. CA19-9 Level to Serum γ-Glutamyltransferase as a Potential Prognostic Biomarker in Patients with Pancreatic Head Carcinoma[J]. Cancer Manag Res, 2021, 13: 4887-4898. doi: 10.2147/CMAR.S313517
[7] Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma[J]. Hepatology, 2018, 67(1): 358-380. doi: 10.1002/hep.29086
[8] 中国抗癌协会肝癌专业委员会, 中华医学会肝病学分会肝癌学组, 中国抗癌协会病理专业委员会, 等. 原发性肝癌规范化病理诊断指南(2015年版)[J]. 中华肝胆外科杂志, 2015, 21(3): 145-151. doi: 10.3760/cma.j.issn.1007-8118.2015.03.001
[9] Amin MB, Edge S, Greene F, et al. AJCC cancer staging manual. 8th ed[M]. New York: Springer, 2017.
[10] 高波, 于晓昌, 傅晓明. 剪切波弹性成像测量肝脏硬度与Child-Pugh分级之间的关系[J]. 现代消化及介入诊疗, 2020, 25(9): 1247-1251. doi: 10.3969/j.issn.1672-2159.2020.09.027
[11] 陆伟, 张占卿, 沈芳, 等. 血清HBsAg和HBV DNA定量水平预测慢性乙型肝炎患者肝组织炎症活动度和纤维化程度的评价[J]. 实用肝脏病杂志, 2016, 19(1): 20-25. doi: 10.3969/j.issn.1672-5069.2016.01.006
[12] Liao R, Fu YP, Wang T, et al. Metavir and FIB-4 scores are associated with patient prognosis after curative hepatectomy in hepatitis B virus-related hepatocellular carcinoma: a retrospective cohort study at two centers in China[J]. Oncotarget, 2017, 8(1): 1774-1787. doi: 10.18632/oncotarget.12152
[13] Chong HH, Yang L, Sheng RF, et al. Multi-scale and multi-parametric radiomics of gadoxetate disodium-enhanced MRI predicts microvascular invasion and outcome in patients with solitary hepatocellular carcinoma ≤ 5 cm[J]. Eur Radiol, 2021, 31(7): 4824-4838. doi: 10.1007/s00330-020-07601-2
[14] Qi LN, Ma L, Wu FX, et al. S100P as a novel biomarker of microvascular invasion and portal vein tumor thrombus in hepatocellular carcinoma[J]. Hepatol Int, 2021, 15(1): 114-126. doi: 10.1007/s12072-020-10130-1
[15] Wu Y, Tu C, Shao C. The value of preoperative systemic immune-inflammation index in predicting vascular invasion of hepatocellular carcinoma: a meta-analysis[J]. Braz J Med Biol Res, 2021, 54(4): e10273. doi: 10.1590/1414-431x202010273
[16] Shi K, Li P, Xue D, et al. Neutrophil-lymphocyte ratio and the risk of hepatocellular carcinoma in patients with hepatitis B-caused cirrhosis[J]. Eur J Gastroenterol Hepatol, 2021, 33(1S Suppl 1): e686-e692.
[17] Johnson PJ, Dhanaraj S, Berhane S, et al. The prognostic and diagnostic significance of the neutrophil-to-lymphocyte ratio in hepatocellular carcinoma: a prospective controlled study[J]. Br J Cancer, 2021, 125(5): 714-716. doi: 10.1038/s41416-021-01445-3
[18] 陈永泰, 柯瑞盛, 蔡秋程, 等. 中性粒细胞/淋巴细胞比值对肝细胞癌患者肝移植术后无复发生存的预测价值[J]. 中华肝胆外科杂志, 2020, 26(11): 821-824. doi: 10.3760/cma.j.cn113884-20200315-00138
[19] Zeng F, Chen B, Zeng J, et al. Preoperative neutrophil-lymphocyte ratio predicts the risk of microvascular invasion in hepatocellular carcinoma: A meta-analysis[J]. Int J Biol Markers, 2019, 34(3): 213-220. doi: 10.1177/1724600819874487
[20] Malhab L, Saber-Ayad MM, Al-Hakm R, et al. Chronic Inflammation and Cancer: The Role of Endothelial Dysfunction and Vascular Inflammation[J]. Curr Pharm Des, 2021, 27(18): 2156-2169. doi: 10.2174/1381612827666210303143442
[21] 韩学艳, 李畅. sssLINC00685和miR-139在肝癌组织中的表达及意义探讨[J]. 中国中西医结合消化杂志, 2020, 28(10): 791-795. doi: 10.3969/j.issn.1671-038X.2020.10.12 http://zxpw.cbpt.cnki.net/WKD2/WebPublication/paperDigest.aspx?paperID=1216e537-b7f2-4edf-a6bb-78fab1362117
[22] Edoo M, Chutturghoon VK, Wusu-Ansah GK, et al. Serum Biomarkers AFP, CEA and CA19-9 Combined Detection for Early Diagnosis of Hepatocellular Carcinoma[J]. Iran J Public Health, 2019, 48(2): 314-322.
[23] Zhang W, Wang Y, Dong X, et al. Elevated serum CA19-9 indicates severe liver inflammation and worse survival after curative resection in hepatitis B-related hepatocellular carcinoma[J]. Biosci Trends, 2022, 15(6): 397-405.
[24] Zhang LX, Lv Y, Xu AM, et al. The prognostic significance of serum gamma-glutamyltransferase levels and AST/ALT in primary hepatic carcinoma[J]. BMC Cancer, 2019, 19(1): 841. doi: 10.1186/s12885-019-6011-8
[25] 赵全能, 李炙莲, 崔学丽, 等. 血清CA19-9评估原发性肝细胞癌微血管侵犯[J]. 西部医学, 2021, 33(12): 1840-1843. doi: 10.3969/j.issn.1672-3511.2021.12.025
[26] Takemura K, Board PG, Koga F. A Systematic Review of Serum γ-Glutamyltransferase as a Prognostic Biomarker in Patients with Genitourinary Cancer[J]. Antioxidants(Basel), 2021, 10(4): 549.
[27] 王芳菲, 吕少诚, 曹迪, 等. 术前CA19-9/GGT比值与远端胆管癌术后远期生存的相关性分析[J]. 中华肝胆外科杂志, 2021, 27(10): 762-766. doi: 10.3760/cma.j.cn113884-20201215-00624
[28] 于洁, 段红亮, 吴晓庆, 等. 原发性肝细胞癌微血管侵犯的术前预测模型构建及临床意义[J]. 中华普外科手术学杂志(电子版), 2021, 15(1): 57-60. doi: 10.3877/cma.j.issn.1674-3946.2021.01.017.
-
图(1)
表(4)
计量
- 文章访问数: 1155
- PDF下载数: 224
- 施引文献: 0