
Construction and validation of a novel nomogram for predicting recurrent choledocholithiasis after ERCP
-
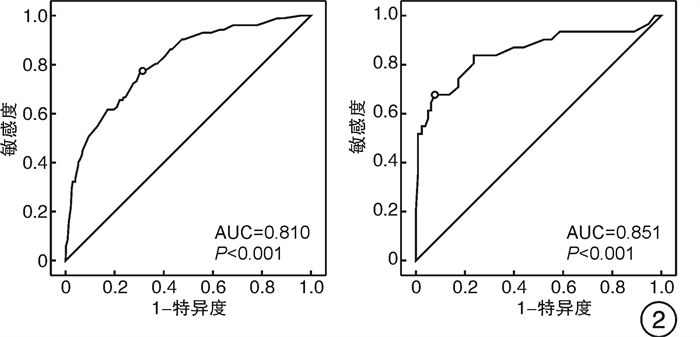
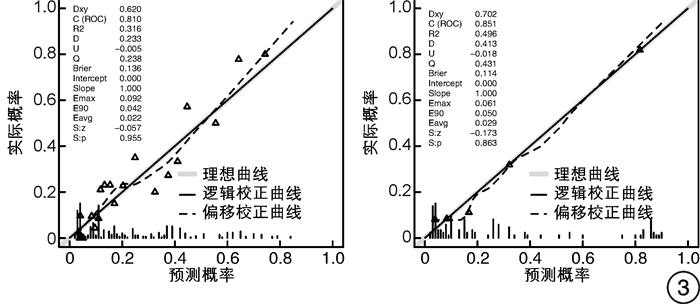
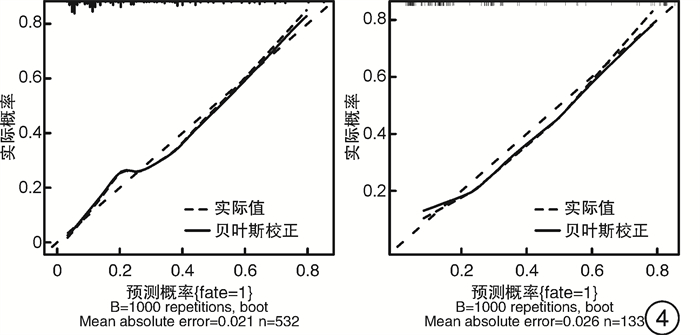
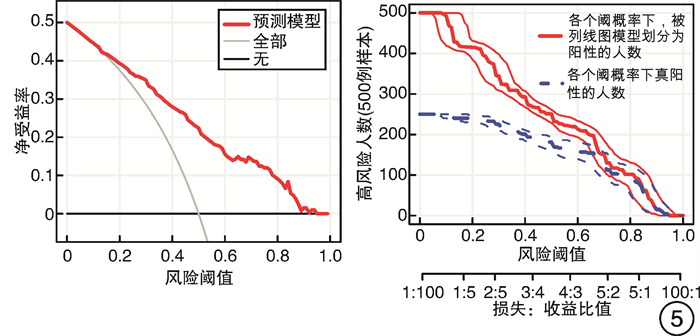
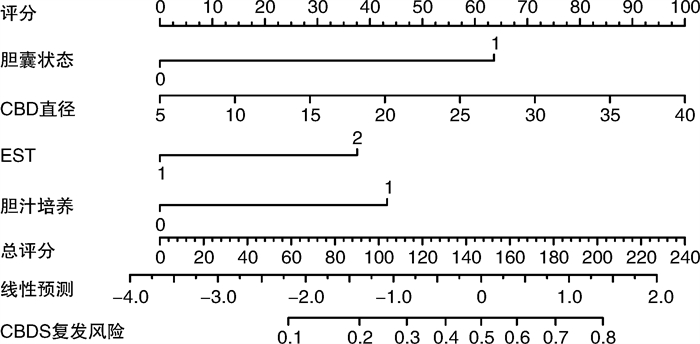
摘要: 目的 探讨经内镜逆行胰胆管造影(ERCP)取石术后胆总管结石(CBDS)复发的危险因素,绘制列线图风险预测模型,并进行验证。方法 选取2017年1月—2020年12月期间于苏州大学附属第一医院消化内科行ERCP治疗的胆总管结石患者共计665例,按照8∶2随机抽取,532例(80%)作为建模组,133例(20%)作为验证组,根据结石是否复发,分为复发组和未复发组,比较2组患者资料差异,运用单因素和多因素分析筛选出ERCP术后胆总管结石复发的独立危险因素,绘制列线图风险预测模型,并进行验证。结果 在建模组532例患者中,131例复发,复发率24.6%。多因素logistic回归分析显示胆囊切除术后、胆总管扩张、胆汁细菌培养阳性、乳头括约肌切开是ERCP术后胆总管结石复发的独立危险因素(P< 0.05)。在建模组和验证组中,列线图模型的C指数和AUC值分别为0.810(95%CI:0.770~0.846)、0.851(95%CI:0.771~0.912),校正C指数分别为0.822、0.862,校正曲线表明预测结果和实际结果之间具有良好的一致性。决策曲线表示该模型有较高的临床应用价值。结论 胆囊切除术后、胆总管扩张、胆汁细菌培养阳性、十二指肠乳头括约肌切开是ERCP术后胆总管结石复发的独立危险因素。本研究构建了一个新型ERCP术后胆总管结石复发的风险预测模型,经验证具有良好的区分度、一致性和临床实用性。
-
关键词:
- 胆总管结石 /
- 复发 /
- 经内镜逆行胰胆管造影术 /
- 列线图 /
- 验证
Abstract: Objective To construct and validate a novel nomogram for predicting recurrent choledocholithiasis after endoscopic retrograde cholangiopancreatography(ERCP).Methods A total of 665 patients with choledocholithiasis who received ERCP treatment were admitted to the First Affiliated Hospital of Soochow University from January 2017 to December 2020. The collected data were randomly divided into a training set(n=532, 80%) and a validation set(n=133, 20%). According to whether the stones recurred, they were divided into the recurrence group and the non recurrence group. The data of the two groups were compared, and the independent risk factors for the recurrence of common bile duct stones after ERCP were screened out by univariate and multivariate analysis. A novel nomogram was established by binary logistic regression based on the training set data. The C-index and the area under the receiver operating characteristic curve(AUC) analysis were used to assess the discrimination of the nomogram. The calibration plot was drawn to evaluate the calibration of the nomogram. The bootstrapping method was performed to calculate the bias-corrected C-index.Results Multivariate logistic regression analysis showed that cholecystectomy, positive bile bacterial culture, common bile duct dilation and sphincterotomy were independent risk factors for common bile duct stone recurrence after ERCP. In the training set, the C-index and the AUC value was 0.810(95%CI: 0.770-0.846). The bias-corrected C-index was 0.822. In the validation set, the C-index and the AUC value was 0.851(95%CI: 0.771-0.912). The bias-corrected C-index was 0.862.Conclusion Cholecystectomy, positive bile bacterial culture, common bile duct dilation and sphincterotomy are independent risk factors for recurrent choledocholithiasis after ERCP. We have constructed and validated a novel nomogram for predicting recurrent choledocholithiasis after ERCP. -

-
表 1 建模组中未复发与复发患者单因素分析
变量 未复发(n=401) 复发(n=131) P 女性/例(%) 172(42.9) 58(44.3) 0.782 年龄>65岁/例(%) 202(50.4) 67(51.1) 0.878 体重指数/(kg/m2) 23.5±3.2 22.6±3.2 0.013 aCCI 3.0(1.0,4.0) 3.0(1.0,4.0) 0.888 WBC/(×109·L-1) 4.6(3.7,7.9) 5.6(4.4,7.8) 0.653 NE/(×109·L-1) 3.6(2.6,5.7) 3.4(2.6,5.5) 0.872 PCT/(ng·mL-1) 0.1(0.0,0.6) 0.1(0.0,0.6) 0.297 TBIL/(μmol·L-1) 22.4(15.2,58.4) 18.6(12.3,32.1) 0.001 ALT/(U·L-1) 74.4(24.7,190.2) 35.0(17.4,120.1) 0.001 AST/(U·L-1) 40.6(21.6,105.3) 27.4(19.4,65.7) 0.002 GGT/(U·L-1) 251.1(83.8,501.6) 172.5(47.1,335.5) 0.001 ALP/(U·L-1) 136.7(91.9,414.7) 111.7(80.9,201.8) 0.007 术后胰腺炎/例(%) 18(4.5) 5(3.8) 0.735 高淀粉酶血症/例(%) 124(30.9) 30(22.9) 0.074 既往胆道手术史/例(%) 37(9.2) 25(19.1) 0.002 胆囊状态/例(%) < 0.001 a 80(20.0) 18(13.7) b 135(33.7) 10(7.6) c 129(32.2) 96(73.3) d 57(14.2) 7(5.3) 术前胆管炎/例(%) 152(37.9) 52(39.7) 0.715 结石数目多发/例(%) 228(56.9) 84(64.1) 0.143 结石直径/mm 8.0(8.0,11.0) 10.0(8.0,15.0) < 0.001 结石位于中下段/例(%) 279(69.6) 92(69.2) 0.385 胆总管直径/mm 12.0(10.0,18.0) 15.0(12.0,18.0) < 0.001 胆汁培养阳性/例(%) 176(52.4) 22(21.6) < 0.001 壶腹周围憩室/例(%) 104(25.9) 31(31.0) 0.604 乳头括约肌切开/例(%) 339(84.5) 51(46.8) < 0.001 乳头切开长度/mm 5.0(3.0,5.0) 5.0(3.0,5.0) 0.034 治疗方式/例(%) < 0.001 EST 58(14.6) 13(19.4) EPBD 57(14.4) 16(23.9) sEST-EPBD 281(71.0) 38(56.7) 胆道支架置入/例(%) 88(22.1) 25(19.1) 0.463 鼻胆管引流/例(%) 322(80.5) 98(74.2) 0.126 注:EST,内镜下乳头括约肌切开术;EPBD,内镜下乳头括约肌球囊扩张术;sEST-EPBD,内镜下乳头括约肌小切开术联合乳头球囊扩张术。  下载: 导出CSV
下载: 导出CSV
表 2 多因素logistic回归分析
变量 OR 95%CI P 胆囊术后 4.581 2.807~7.477 <0.001 胆总管直径 1.088 1.037~1.141 0.001 乳头括约肌切开 2.833 1.429~3.802 0.001 胆汁细菌培养阳性 2.611 1.513~4.525 0.001
下载: 导出CSV
-
[1] Cai JS, Qiang S, Bao-Bing Y. Advances of recurrent risk factors and management of choledocholithiasis[J]. Scand J Gastroenterol, 2017, 52(1): 34-43. doi: 10.1080/00365521.2016.1224382
[2] ASGE Standards of Practice Committee, Buxbaum JL, Abbas Fehmi SM, et al. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis[J]. Gastrointest Endosc, 2019, 89(6): 1075-1105.e15. doi: 10.1016/j.gie.2018.10.001
[3] Wu Y, Xu CJ, Xu SF. Advances in Risk Factors for Recurrence of Common Bile Duct Stones[J]. Int J Med Sci, 2021, 18(4): 1067-1074. doi: 10.7150/ijms.52974
[4] Oak JH, Paik CN, Chung WC, et al. Risk factors for recurrence of symptomatic common bile duct stones after cholecystectomy[J]. Gastroenterol Res Pract, 2012, 2012: 417821.
[5] Li S, Su B, Chen P, et al. Risk factors for recurrence of common bile duct stones after endoscopic biliary sphincterotomy[J]. J Int Med Res, 2018, 46(7): 2595-2605. doi: 10.1177/0300060518765605
[6] Park SY, Hong TH, Lee SK, et al. Recurrence of common bile duct stones following laparoscopic common bile duct exploration: a multicenter study[J]. J Hepatobiliary Pancreat Sci, 2019, 26(12): 578-582. doi: 10.1002/jhbp.675
[7] Yoo ES, Yoo BM, Kim JH, et al. Evaluation of risk factors for recurrent primary common bile duct stone in patients with cholecystectomy[J]. Scand J Gastroenterol, 2018, 53(4): 466-470. doi: 10.1080/00365521.2018.1438507
[8] Park BK, Seo JH, Jeon HH, et al. A nationwide population-based study of common bile duct stone recurrence after endoscopic stone removal in Korea[J]. J Gastroenterol, 2018, 53(5): 670-678. doi: 10.1007/s00535-017-1419-x
[9] Zhang R, Luo H, Pan Y, et al. Rate of duodenal-biliary reflux increases in patients with recurrent common bile duct stones: evidence from barium meal examination[J]. Gastrointest Endosc, 2015, 82(4): 660-665. doi: 10.1016/j.gie.2015.03.1908
[10] Konstantakis C, Triantos C, Theopistos V, et al. Recurrence of choledocholithiasis following endoscopic bile duct clearance: Long term results and factors associated with recurrent bile duct stones[J]. World J Gastrointest Endosc, 2017, 9(1): 26-33. doi: 10.4253/wjge.v9.i1.26
[11] Paspatis GA, Paraskeva K, Vardas E, et al. Long-term recurrence of bile duct stones after endoscopic papillary large balloon dilation with sphincterotomy: 4-year extended follow-up of a randomized trial[J]. Surg Endosc, 2017, 31(2): 650-655. doi: 10.1007/s00464-016-5012-9
[12] 黄瑶, 易剑锋, 周文策. 胆总管结石治疗后复发因素的研究进展[J]. 中国普通外科杂志, 2021, 30(8): 964-970. https://www.cnki.com.cn/Article/CJFDTOTAL-ZPWZ202108012.htm
[13] 王士东. ERCP取石术后胆总管结石复发的相关因素分析[D]. 青岛: 青岛大学, 2020.
[14] Keizman D, Shalom MI, Konikoff FM. An angulated common bile duct predisposes to recurrent symptomatic bile duct stones after endoscopic stone extraction[J]. Surg Endosc, 2006, 20(10): 1594-1599. doi: 10.1007/s00464-005-0656-x
[15] Nzenza TC, Al-Habbal Y, Guerra GR, et al. Recurrent common bile duct stones as a late complication of endoscopic sphincterotomy[J]. BMC Gastroenterol, 2018, 18(1): 39. doi: 10.1186/s12876-018-0765-3
[16] Gulubov MV, Hadjipetkov P, Sivrev D, et al. Endocrine cells in the human common bile duct in patients with obstructive jaundice[J]. Hepatogastroenterology, 2012, 59(113): 26-30.
[17] Jeon J, Lim SU, Park CH, et al. Restoration of common bile duct diameter within 2 weeks after endoscopic stone retraction is a preventive factor for stone recurrence[J]. Hepatobiliary Pancreat Dis Int, 2018, 17(3): 251-256. doi: 10.1016/j.hbpd.2018.03.014
[18] Deng F, Zhou M, Liu PP, et al. Causes associated with recurrent choledocholithiasis following therapeutic endoscopic retrograde cholangiopancreatography: A large sample sized retrospective study[J]. World J Clin Cases, 2019, 7(9): 1028-1037. doi: 10.12998/wjcc.v7.i9.1028
[19] 郝志远. 胆总管结石合并胆管炎肠道微生态宏基因组测序及代谢组学分析[D]. 上海: 中国人民解放军海军军医大学, 2021.
[20] 王志毅. 胆总管结石合并胆囊结石经ERCP联合LC后胆总管结石复发的危险因素分析[D]. 苏州: 苏州大学, 2020.
[21] Wu SD, Uchiyama K, Fan Y. The role and mechanism of fatty acids in gallstones[J]. Hepatobiliary Pancreat Dis Int, 2007, 6(4): 399-401.
[22] 李静, 苗龙, 周文策. 消化道微生态与胆结石疾病关系的研究进展[J]. 中国普通外科杂志, 2020, 29(8): 1000-1005. https://www.cnki.com.cn/Article/CJFDTOTAL-ZPWZ202008016.htm
[23] Tsai TJ, Lin CK, Lai KH, et al. Does preserved sphincter of Oddi function prevent common bile duct stones recurrence in patients after endoscopic papillary balloon dilation?[J]. J Chin Med Assoc, 2018, 81(4): 311-315. doi: 10.1016/j.jcma.2018.01.007
[24] Minakari M, Samani RR, Shavakhi A, et al. Endoscopic papillary balloon dilatation in comparison with endoscopic sphincterotomy for the treatment of large common bile duct stone[J]. Adv Biomed Res, 2013, 2: 46. doi: 10.4103/2277-9175.114186
[25] Ryozawa S, Itoi T, Katanuma A, et al. Japan Gastroenterological Endoscopy Society guidelines for endoscopic sphincterotomy[J]. Dig Endosc, 2018, 30(2): 149-173. doi: 10.1111/den.13001
[26] Yamamoto R, Tazuma S, Kanno K, et al. Ursodeoxycholic acid after bile duct stone removal and risk factors for recurrence: a randomized trial[J]. J Hepatobiliary Pancreat Sci, 2016, 23(2): 132-136. doi: 10.1002/jhbp.316
[27] 李志晋, 徐燕琴, 洪丽华, 等. 鼻胆管灌注柴胡四金汤对预防胆总管结石ERCP术后复发的效果观察[J]. 江西医药, 2021, 56(9): 1540-1542. doi: 10.3969/j.issn.1006-2238.2021.09.072
[28] Fukuba N, Ishihara S, Sonoyama H, et al. Proton pump inhibitor is a risk factor for recurrence of common bile duct stones after endoscopic sphincterotomy-propensity score matching analysis[J]. Endosc Int Open, 2017, 5(4): E291-E296. doi: 10.1055/s-0043-102936
[29] Uchida N, Hamaya S, Tatsuta M, et al. Extracorporeal abdominal massage may help prevent recurrent bile duct stones after endoscopic sphincterotomy[J]. Endosc Int Open, 2016, 4(8): E870-E873. doi: 10.1055/s-0042-109774
[30] Di Ciaula A, Garruti G, Frühbeck G, et al. The Role of Diet in the Pathogenesis of Cholesterol Gallstones[J]. Curr Med Chem, 2019, 26(19): 3620-3638. doi: 10.2174/0929867324666170530080636
-
图(5)
表(2)
计量
- 文章访问数: 1276
- PDF下载数: 1394
- 施引文献: 0